I thought I would take screenshots of my application for future trainees to help them while applying for speciality training. Please find them attached below. I can be contacted for any questions on twitter.
Hope this is helpful. Do reply in the comments if there are any questions.
This could be a very short post because the simple answer to this question is that I passed PACES first time with 96% with LUCK. This is an extremely true statement that maybe a lot of people do not realise and if they do, they do not emphasise this to their colleagues. Partly because people like to portray this exam as some amazing feat of skill and perfect clinical examination whereas the reality is a bit like this: you will feel unprepared on the day, you will feel like you have not done enough, you will not be able to complete your neurological examination in time (unless its cranial nerve examination or single command like examination of upper limbs for myotonic dystrophy), you will mess up at parts and you will feel like the examiners are trying to find ways to fail you. After the exam, you will feel like you failed. As with all practical exams, it is worth preparing properly and just going for it because the outcome will be dependent on so many factors, many of which are uncontrollable. I feel like this would take away a lot of the apprehension associated with this exam if people realised how many factors are out of their control.
Having said that, there are certain risk factors that are modifiable and despite luck counting for a lot you can tip the scales in your favour. This is how:
Find a practice partner: Accountability and the Hawthorne effect. This is quite practical – we are all better versions of ourselves when our performance is being observed (usually). This may not apply to everyone as for some of us our performance may be worse. Regardless, having a practice partner who can quiz you and give you feedback on the mistakes you make unconsciously is extremely helpful for both types of people. For the former, it is valuable practice. For people who fall in the second category, it is practice for what is going to a formal examination with people observing you.
Spend time at the hospital:I spent 5 weeks practicing for PACES, every day after work I used to go around with my practice partner and a colleague who had very kindly volunteered to examine us on cases. We took it upon ourselves to find cases and examine every day to improve our clinical skill and time management (which is an underrated part of prep work for this exam). You need to get better at picking up clinical signs but you also need to get better at picking up those signs quickly. Learn to understand the higher value of some aspects of clinical examination compared to others. Inspection and observing the patient before diving in to examine can give you many clues.
Use Pastest videos: For £130, I got access to some valuable videos which I used to watch whenever I did not feel like studying for the exam. I would highly recommend these.
Work on your presentation skills more than your examination, but also work on your examination:If you carry out a thorough clinical examination but are not able to put together your findings in a concise summary to present – you are doing yourself a disservice. Practice presenting as much as you practice examining because this will embellish your performance. Do not discount the importance of this.
Use Cases for PACES and go for a PACES course: Excellent book. Has everything you need to pass the exam if utilised enough. I went for the PassPACES course (expensive, £1400 but my deanery paid for it as I was a trainee) which was extremely helpful. I saw a case on the course that was in Station 5 and I would not have passed without it.
Give yourself enough time (but not too much): I was forced due to my personal circumstances (and a fear of examinations getting cancelled due to Covid) to prep in 5 weeks for PACES. If you can, give yourself enough time and make a time table before you start your revision. The other thing worth considering is that you do not want to give yourself too much time because this can ramp up anxiety levels and once you feel almost ready you do not want to wait too long. Find the sweet spot.
Accept the stress, it is a driver:Acute stress is good for us (mostly) as it improves academic performance and cognitive drive. Accept the stress and work with it. The problem is when this stress starts to snowball and becomes overwhelming.
Consider your personal circumstances: Can you realistically sit the exam with your current financial and personal responsibilities? Would it be better to plan for a few months, save up and then sit the exam? These are questions worth asking yourself. The revision for PACES is a stressful time, you do not need to add to your worries by doing the exam in a time where your time and money is required elsewhere. I revised with a 4-month-old baby – I was only able to do this because my wife was amazing and supported me throughout. I also planned ahead and worked extra shifts to save up for it. So plan ahead and consider your circumstances.
Do what you can, do not worry about the rest: You can only do what you can do. This advice should apply to things beyond this exam as well. Focus on the factors you can control, like the ones mentioned in this post, try and ignore the ones that are outside your control. It will not improve your preparation – only hamper it.
Be patient with the result, failing this exam is not the end of the world: The best doctors I have worked with have failed PACES once, or maybe more than that. It says absolutely nothing about your clinical skill and is not a benchmark for the type of doctor you are. It says nothing about how safe you are or about how good a leader you are. It is an exam based on reproduction of learned behaviours and communication skills – however I will say the preparation for this makes you a better doctor. The most recent statistics from the annual performance report 2020 make for interesting reading: “Female candidates have higher pass rates than Male candidates and White candidates have higher pass rates than BAME, for both UK trainees and other candidate groups.” Statistically, I was in the worst category for PACES – Male, International Medical Graduate (IMG) and non-white but luckily and with some hard work I managed to pass the exam. Do your best and if it doesn’t work out – take the exam again. All the best with everything and hope this is helpful. If I missed out on things, please let me know in the comments!
References
(A) Bessant R, Bessant D, Chesser A, Coakley G. Analysis of predictors of success in the MRCP (UK) PACES examination in candidates attending a revision course. Postgrad Med J. 2006;82(964):145-149. doi:10.1136/pmj.2005.035998 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2596701/)
I completed Core Medical Training in July/August 2020 in the middle of the Covid pandemic. I had decided what I wanted to do towards the end of my CT1 – I knew I wanted to specialise in Clinical Oncology. As this is a competitive speciality, my intention was to work on my portfolio however this was made difficult by having to do 3 exams – MRCP I, II and PACES within a very short space of time (I sat and passed my PACES just before the pandemic kicked off) – made it very difficult to dedicate myself to portfolio improvement.
At the time, I was focused on getting an ST3 number and was very disappointed when I did not get into Oncology. This was also in part due to the fact that the entire recruitment system was based on self-assessment (my interview was cancelled the night before I was due to travel to London due to the Prime Minister’s announcement) In retrospect however, this is the best thing that happened to me and my family and I will elaborate why. I remember under-scoring myself too because I was afraid of over-scoring whereas I now think I could have claimed a lot more marks for my achievements. I was offered a job as a Geriatric Medicine / Acute Oncology SpR which was perfect for my career development and therefore I accepted it.
I was also aware that due to my personal circumstances, (my wife had a training number in Wessex and now KSS and my son was 18 months old) I could not just pick up my bags and move to wherever I was offered an ST3 post. I picked up a map and drew a circle around the possible areas I could possibly commute to (I was already doing a 64-mile commute every day for the last 3 years so this would not be a problem for me) and then divided that circle into two halves to set my priorities for locations. A referred to my first-choice locations and B referred to my second-choice locations. Everything else would have to be after these and I knew I would refuse the other places if they were offered to me.
These are the reasons I would recommend a year as a Geriatric Medicine SpR to everyone post-CMT (or a year in your chosen speciality without on-calls):
A well-deserved break
This is the most important thing in my opinion. I remember being exhausted at the end of my CMT, having done 3 exams in 1 year (MRCP I, II and PACES all within the span of 13 months). If I had gone straight into ST3, I would have struggled and most likely be facing burnout with no break and incredibly hectic training rotas with the increasingly demanding portfolio requirements that come with these. Another factor that has been an issue for international medical graduates (IMGs) like me is that I have not seen my parents in 2 years. The pandemic has had such a massive impact on so many people and one of the ways it has impacted IMGs is that due to the financial impact or other considerations of multiple countries being red-listed, we have not been able to see our loved ones. The mental health impact of this must not be under-estimated. A break from a hectic routine to focus on improving other aspects of our life – sleep, diet, exercise and time with family and friends cannot be recommended enough. I did all of this having a son who was a year old and a wife who also had a busy rotation in Emergency Medicine post-maternity leave. I was able to do all pick ups and drop offs and did all the bedtimes with my son for the first 6 months after my wife went back to work. None of this would have been possible if I was on a busy on-call rota.
Confidence in making decisions
I worked as a Medical SpR towards the end of my CMT especially after I had passed PACES, stepping up when needed to cover shifts. Initially this was under supervision with the SpRs on-call while I was CT2 however soon I progressed to working independently. One of the most important factors behind this was because I had consistently volunteered to undertake difficult conversations and manage complex cases which gave me a lot of confidence in my abilities. Working as a Geriatric SpR, I gained amazing amounts of confidence making multiple small decisions every day, leading ward rounds and being in charge for junior colleagues on the wards. This degree of confidence is difficult to obtain unless you make multiple decision everyday which relate to patient care and can impact the patient journey. While this is a scary aspect for most of us, if you start off doing this on a ward-based setting, it is generally safer compared to starting off with GIM on-calls where there is less safety-netting. This did not apply to me but I still feel it is worth mentioning.
You can make this year what you want – you have time to improve your portfolio with no commitments
I was told this by one of my consultants that this year could be whatever I made it out to be. This turned out to be exactly the case – I used this year to write the protocol for Cancer associated thrombosis in my trust, co-authored the entire VTE guideline for the hospital and improved my portfolio significantly which granted me a much better chance of success at my ST3 application. I talked about my achievements at my interview and this would not have been possible if I had spent my time doing on-calls. I devised a rota for myself and stuck to that diligently, doing clinics and spending time on an honorary contract at a local cancer centre. I observed radiotherapy delivery and planning on my study leave as well. I wrote other guidelines in my trust and became involved in management work. I published a rare case as a first author in a PubMed indexed journal.
Being able to prognosticate without being on-call
Working specifically in a Geriatric Medicine ward means having to make decisions being the most senior member of the team at times, especially during the afternoon. This is usually about sick patients who need a decision regarding the potential reversibility of their medical problems vs their frailty and you become a lot more comfortable with making the tough decisions. One of the under-recognized benefits would be the improvement of your communication skills as a by-product of having to have tough conversations repeatedly. Normally, you are exposed to a lot of this when you are on-call however being a SpR in Geriatric Medicine gives you a chance to experience all of that without the time-commitment.
More time for clinics
No brainer – not doing on-calls gives you more time for clinics which directly improve your knowledge about specialist management.
Exploration of other options (if unsure)
When I was trying to decide my speciality options, I was trying to decide between Oncology, Rheumatology and Acute Medicine/Intensive care. As I spent more time in Core Medical Training and having gone through an intensive care rotation, I gained more experience in these specialities and finally decided my speciality path. However, if someone is unsure about what they want to do, a year without any on-call commitments can be a very useful thing to tailor your interests and decide on your path.
I am aware this may not be possible for everyone and even the ability to take time off the on-call rota by choice is a privilege that I have:
It may not be possible if you cannot afford to take a hit to your salary – I did this knowing my wife and I were both working, and we had to share childcare duties. If she was not working, I would not have taken time off the on-call rota.
It may not be the best idea if you are aiming to get into a less competitive speciality (especially with IMT3 now) – this is important if you are aiming to get into Acute Medicine/Geriatric Medicine which are the general medical specialities and are comparatively less competitive. If you want to take time to improve your CV by doing ultrasound or simulation as a sub-speciality interest, I think it would be better done by taking an OOPY as detailed here: https://www.jrcptb.org.uk/training-certification/out-programme
It is probably not suitable if you are not willing to leave out the on-call experience for working on your portfolio. It is a trade off at the end of the day. You get less WPBAs done due to seeing less acute patients but you can work on research/guideline writing/management stuff as detailed above.
It may not be suitable if you have student loans to think of or other financial responsibilities as discussed.
Please let me know if there is anything else I have missed. As always, there will be people who will disagree with this and that is okay. This is just my experience. All the best!
This post is meant to highlight how I got a ClinOnc ST3 number in my first-choice deanery, improved my score 90 points in 1 year (114th to 24th nationally) and got into my first-choice deanery. This will focus on the actual breakdown of the interview + self-assessment. In order to see my other posts, please visit my blog: https://oncologydoc.wordpress.com/
Unfortunately, despite attempting to find guidance regarding the exact breakdown for interview and self-assessment weightage I did not have much luck. But as a simple guide, portfolio/self-assessment score is very important, and all attempts must be made to maximize score in this section, but the interview counts for more and would be the differentiating factor in your rank.
I first applied for ST3 Clinical Oncology towards the end of my Core Medical Training in August, 2020. Due to the first wave of the Covid-19 pandemic, there were no interviews and the application self-assessment was the only factor that determined your ST3 rank. I ranked 114th nationally in this round and I felt this was because:
I under-scored myself due to my anxiety about over-scoring myself
I am the sort of person who interviews well and I believe I would have had a much better rank if interviews went ahead
I was not able to claim for certain things that were achieved after shortlisting
At the moment, this felt like a disappointment but on reflection this was the best thing that could have happened to me. I have detailed why here.
There are 10 sections to the portfolio (this may vary between specialities) and self-assessment scoring algorithm. The sections are detailed below:
(a) Undergraduate: I claimed 0 marks for this as I did not have any undergraduate degrees.
(b) Postgraduate: I claimed 0 marks for this as I had no PG degrees apart from the MRCP (UK).
(c) Prizes/Awards: I self-scored 2 for my distinction in Biochemistry however this was corrected by the reviewers on the grounds that distinction is not included as a prize and this needs to be a first-place prize for undergraduate medicine. I felt this was unfair especially as I got the points for the exact same thing in my Medical Oncology application but the appeals process seemed to be very complex and I chose not to do this.
(d) Presentations: I scored myself 6 points because I had presented an original posted at a National conference on Quality Improvement in London and I had evidence for this – a poster as well as a certificate. The image from ST3 recruitment shows 5 points however the application form had certain changes this year and I got 6 points. I suspect this was because the mark scheme was changed due to the Covid-19 pandemic but these screenshots from the ST3 recruitment website are still a good general guide.
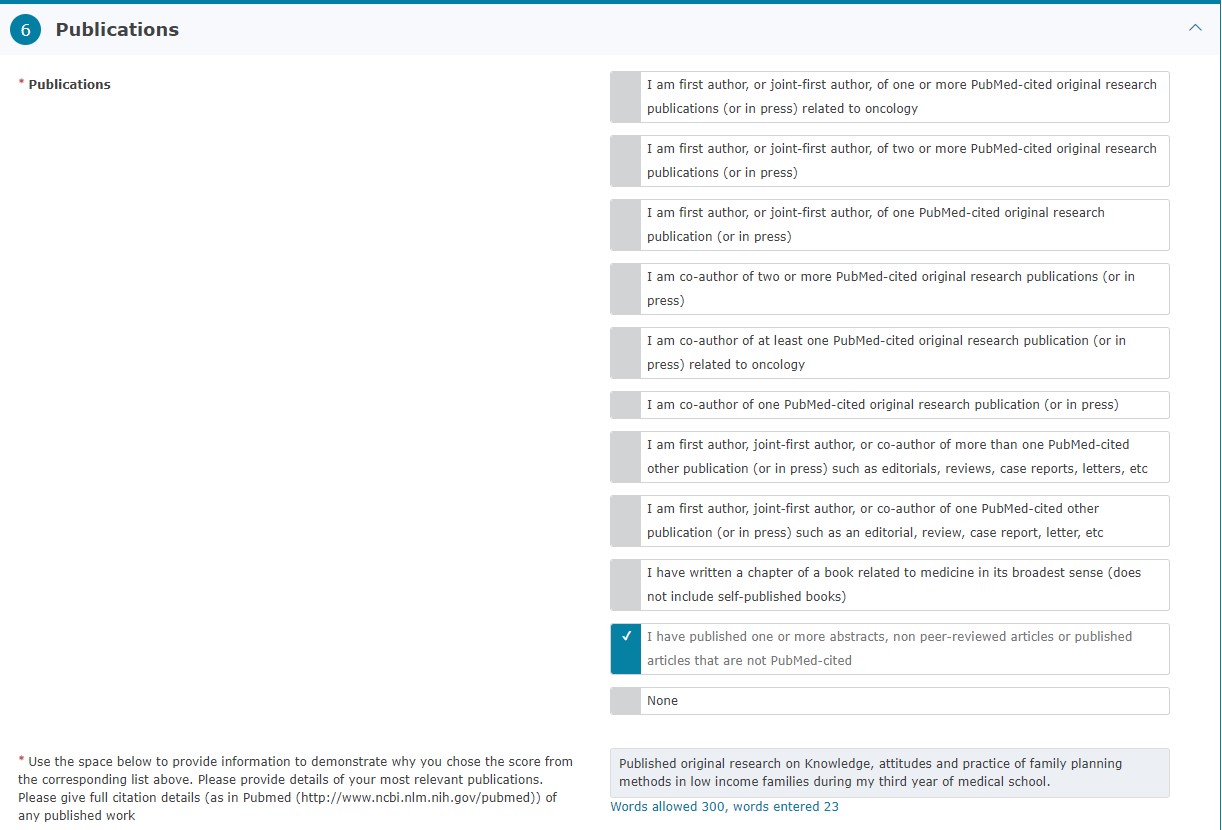
(e) Publications: I claimed 3 points for publishing one article in a non-PubMed-cited journal. After my interview, I published a rare case report on PubMed however this was not completed by the time I had my interview.
(f) Teaching Experience: I claimed 7 points for this which was the maximum number of points possible – this was because I had been leading the local undergraduate teaching programme in my trust for 3 years. This involved setting up curriculum as well as liaising with the College Tutor and arranging teaching sessions, organizing speakers and obtaining regular feedback.
(g) Training in teaching: I claimed 2 points for this because I had 3 days of training in teaching methods – Mentorship workshop (1 day) and teach the teacher course (2 days).
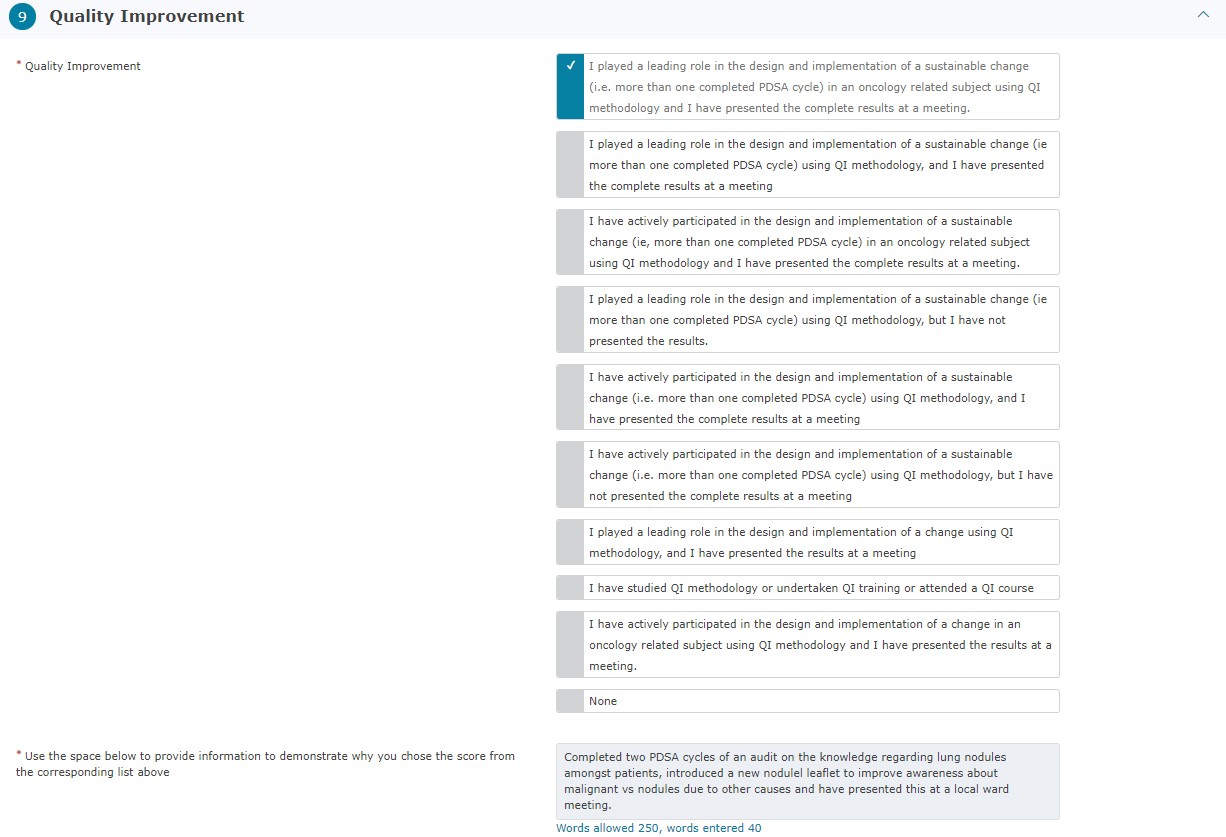
(h) Quality Improvement: I claimed maximum marks in this category – 12 because I had done a project on the assessment of patient satisfaction regarding the management of their lung nodules in my trust and this met the criteria – “I played a leading role in the design and implementation of a sustainable change (i.e. more than one completed PDSA cycle) in an oncology related subject using QI methodology and I have presented the complete results at a meeting.”
I had evidence for this given to me in the form of a letter by the supervising consultant as well as a certificate.
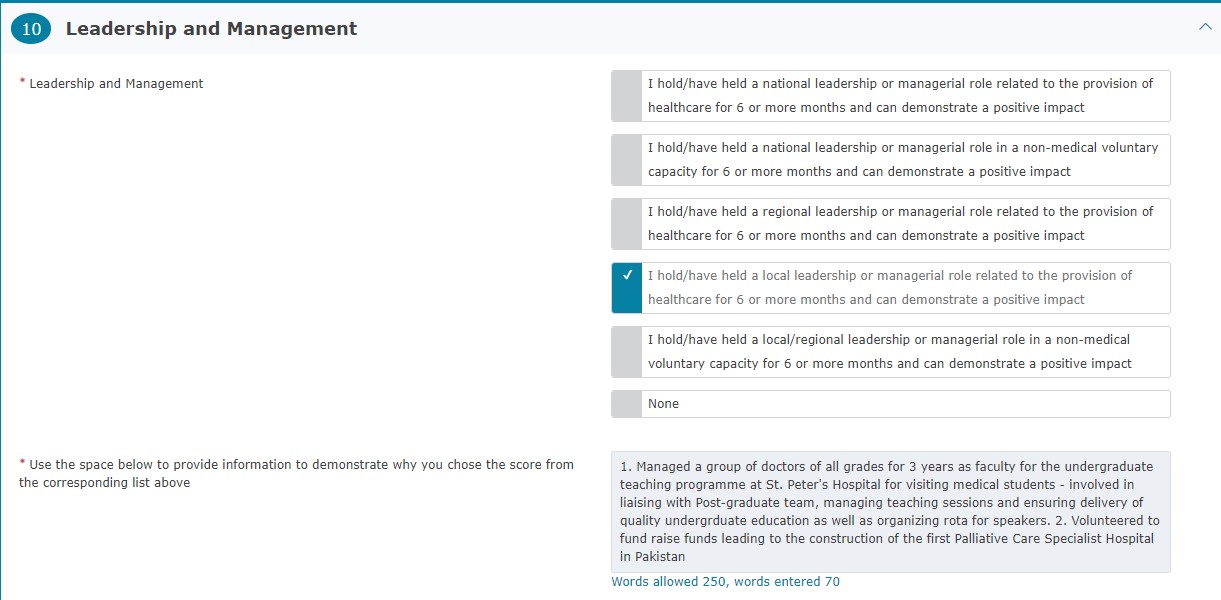
(i) Leadership and management: This got me 4 points as I claimed for my leadership role in providing medical education to undergraduate students – this was a role I had held for 3 years (>6 months gets you marks) and was easy to provide evidence for.
My raw interview score was 34/71 which translates to 47.9%. Even though this is not a bad score at all, this is still not an excellent score and without a solid interview showing I would not have been able to get a spot in my preferred location. My personal circumstances which I also discuss in my article here meant that I could not take any training numbers that were away from London or KSS. This made for a very difficult situation to consider however it worked out in the end as I scored 95% on my interview and my combined score was good enough to rank in the top 20 candidates nationally. This was an improvement of 90 points on my score the year before and the points above are how I managed to do this. As long as you look at the ST3 recruitment page for your speciality and plan accordingly, your goal to get into any speciality should be achievable.
I frequently get asked this question by my colleagues – what are the differences between clinical and medical oncologists? It is easier to explain if we break it down. First, a little bit of information and references that may be useful:
The health careers NHS website is brilliant for understanding the basic job roles (click on link to follow):
The simple explanation is that clinical oncologists deal primarily with radiotherapy and are trained in the science of planning and delivering radiotherapy (curative/neo-adjuvant/adjuvant/palliative). Medical oncologists do not deliver radiotherapy and are not trained for this. Both deal with elements of chemotherapy/immunotherapy however this falls primarily under the medical oncologists domain. Both deal with non-surgical methods of management of malignant diseases.
There is obviously a lot of overlap between the specialities, they are very academic (medical > clinical) and both specialities work in close liaison with each other – sharing the Acute Oncology service in the UK in most centres and in close liaison with the Palliative care teams. Working in both specialities includes working with the Macmillan nurses – who are fantastic and play a huge role in patient care when it comes to Oncology or Palliative care in the UK.
I have listed the other differences in the table below:
Clinical Oncology
Medical Oncology
Under the Royal College of Radiologists
Under the Royal College of Physicians
Pass FRCR examination on their way to becoming consultant in the UK – FRCR Part A divided into 4 modules: cancer biology and radiobiology, clinical pharmacology, physics and medical statistics. This is followed by FRCR Part 2A and 2B
Have to pass Speciality Certificate Examination (SCE) which is a single exam
Deal primarily with radiotherapy / brachytherapy and radiological treatment options as well as some non-radiological treatment options
Deal primarily with non-radiological means of treatment – chemotherapy, immunotherapy, etc
Table: Differences between Clinical and Medical Oncology
This post by Dr. Jeanette Dickinson is excellent reading to get a grasp of the scope of practice for both in the UK. Overall both specialities require excellent communication skills due to the nature of the job. I would suggest strongly considering the Haemato-oncological specialities if you’re interested in exercising your brain as there are not many procedures that are a part of the speciality. Some Palliative care SpRs do specialise in ultrasound so they can insert Ascitic drain or perform Dopplers for DVT to avoid admission to hospital so this could be a potential niche if someone wanted to develop it however I do not know anyone in Oncology who is doing this (so far). There is a variety of clinical conditions that are managed in close liaison with other specialists in an MDT setting. The main differences are summarized in the table above but there are differences in the working patterns of individual trainees which can be better understood by speaking to people in the speciality.
I aim to gather further content from Oncology trainees about their work-life balance and daily routines and publish this here. Please keep an eye on the blog and let me know if I have missed anything!












You must be logged in to post a comment.